Healthy Signs
Healthy Signs
The Affordable Care Act is deeply flawed, but it has nonetheless made healthcare cheaper and more accessible for millions.

The Affordable Care Act, now entering its fifth year of full implementation, is a spectacularly imperfect solution to our healthcare crisis. Many of its imperfections were hard-wired into the original legislation, whose deference to the expectation of job-based coverage, to the panacea of “competition,” and to the actuarial whims of private insurers effectively made the healthcare system’s signal flaws the building blocks of reform. While it survived the GOP’s fetish for repeal, the ACA’s reach and impact has been whittled away by the Supreme Court’s decision to allow states to opt out of Medicaid expansion, by the repeal of the “individual mandate” in the 2016 tax bill, and by the petty sabotage of the Trump administration—including the effort to back out of federal commitments to cost sharing, an executive order blessing the sale of junk insurance products, and the defunding of the ACA’s outreach and enrollment efforts.
Despite its flaws, and against these odds, the ACA has made healthcare cheaper and more accessible. The uninsured rate has fallen by almost half since 2010 (from almost 16 percent to just over 8 percent), although those gains are starting to slow or reverse. While insurance premiums have been volatile, Medicaid expansion and subsidized marketplace plans have dampened out-of-pocket health spending and alleviated some sources of health insecurity. And new coverage, unsurprisingly, has improved health outcomes as more of those who need care get it, and get it earlier.
The uneven expansion of Medicaid undercut these gains, creating a substantial coverage gap for those whose incomes are above their states’ Medicaid eligibility limits but below the lower limit for ACA Marketplace premium tax credits. This created (or left untouched) some yawning regional and racial disparities: 89 percent of those in the coverage gap live in the South (46 percent in Florida and Texas alone), and nearly half are people of color.
At the same time, the uneven Medicaid expansion became a real-time experiment in policy evaluation. If all states had expanded Medicaid, our assessment of the ACA and its impacts would necessarily rely on before-and-after comparisons of coverage, costs, access, and outcomes. Such analysis is important but clumsy, as so many other factors (including recovery from the Great Recession) shaped or confounded these health metrics across the same span.
The decision of some states not to take up the Medicaid expansion (aside from the very real burden it imposed on their citizens) created a sort of lottery, especially for low-income adults without children. This gives us the opportunity to assess the ACA not just over time, but across jurisdictions; to exploit the variation in state policy choice to assess the impact of the ACA’s Medicaid expansion.
The graphic below offers a glimpse of that ongoing assessment, drawing on the work of ACA watchdogs like the Kaiser Family Foundation and the Commonwealth Fund, and on the burgeoning academic research on the ACA’s impact. The graphic draws on studies that make explicit comparisons between expansion and non-expansion states. It shows disparities in a variety of health indicators between states that either took up or rejected Medicaid expansion, and also changes in those indicators before and after the ACA rollout.
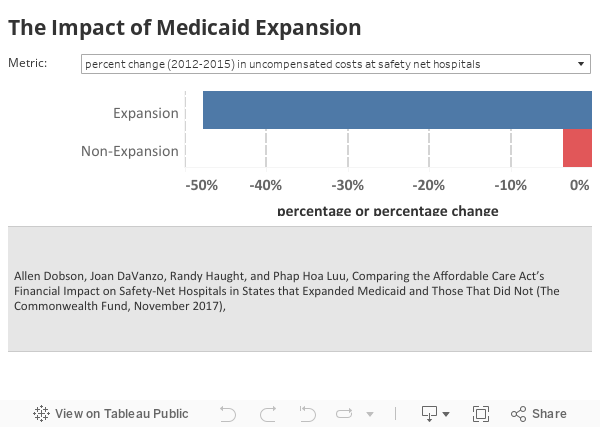
The top-line results are pretty clear: the ACA (and specifically its Medicaid expansion) have led to demonstrable and in some cases dramatic improvements in healthcare coverage, especially for some vulnerable populations. Low-income residents of “expansion” states have better access to healthcare services and providers. And, as a result, those states are starting to see better health outcomes—both on conventional health and clinical metrics, and on self-reported assessments.
What those states are not seeing is just as important: the GOP’s chicken-little conviction that this “job-killing government takeover of healthcare” would be a “train wreck” for the healthcare system and “crush the economy like a ton of bricks.” The ACA has had no discernible impact on employment, apart from adding tens of thousands of new jobs in healthcare. The infusion of federal dollars (the Medicaid expansion costs the states almost nothing) has been a boon to both state budgets and the bottom line of “safety net” hospitals (those that provide care to all patients, regardless of their ability to pay).
Faced with this mounting evidence, it is little wonder that citizens in Idaho, Utah, and Nebraska—three “non-expansion” states that voted overwhelmingly for Trump in 2016—all handily approved ballot measures in November to expand Medicaid. On a less hopeful note, the push to attach work requirements to Medicaid (in expansion and non-expansion states alike) threatens to push up to four million of those currently covered back into the ranks of the uninsured.
Colin Gordon is a professor of history at the University of Iowa. He writes widely on the history of American public policy and is the author, most recently, of Growing Apart: A Political History of American Inequality and Citizen Brown: Race, Democracy, and Inequality in the St. Louis Suburbs (forthcoming, University of Chicago Press).